
 The initial diagnosis of acute coronary syndrome (ACS) is based on history, risk factors, and, to a lesser extent, ECG findings. The symptoms are due to myocardial ischemia, the underlying cause of which is an imbalance between supply and demand of myocardial oxygen.
The initial diagnosis of acute coronary syndrome (ACS) is based on history, risk factors, and, to a lesser extent, ECG findings. The symptoms are due to myocardial ischemia, the underlying cause of which is an imbalance between supply and demand of myocardial oxygen.Patients with ACS include those whose clinical presentations cover the following range of diagnoses: unstable angina, non–ST-elevation myocardial infarction (NSTEMI), and ST-elevation myocardial infarction (STEMI). This ACS spectrum concept is a useful framework for developing therapeutic strategies.
A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after eating a large meal. Pain is now present but is minimal. Aspirin is the single drug that will have the greatest potential impact on subsequent morbidity. In the setting of ongoing symptoms and ECG changes, nitrates titrated to 10% reduction in blood pressure and symptoms, beta-blockers, and heparin are all indicated. If the patient continues to have persistent signs and/or symptoms of ischemia, addition of a glycoprotein IIb/IIIa inhibitor should be considered.


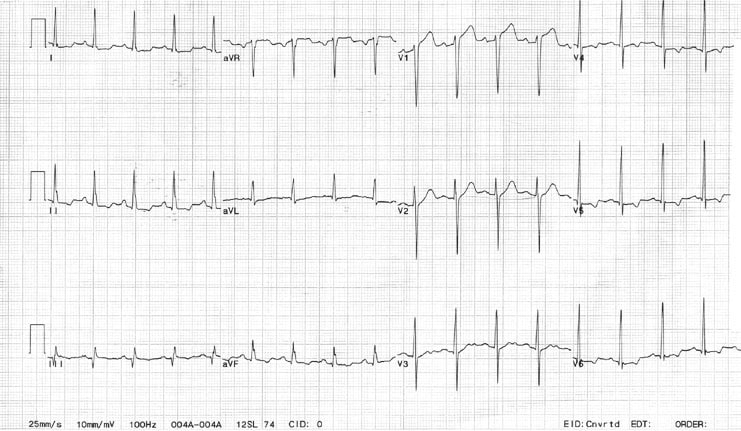
A 62-year-old woman with a history of chronic stable angina and a "valve problem" presents with new chest pain. She is symptomatic on arrival, complaining of shortness of breath and precordial chest tightness. Her initial vital signs are blood pressure 140/90 mm Hg and heart rate is 98. Her ECG is as shown. She is given nitroglycerin sublingually, and her pressure decreases to 80/palpation. Right ventricular ischemia should be considered in this patient.

Pathophysiology
Myocardial ischemia is most often due to atherosclerotic plaques, which reduce the blood supply to a portion of myocardium. Initially, the plaques allow sufficient blood flow to match myocardial demand. When myocardial demand increases, the areas of narrowing may become clinically significant and precipitate angina. Angina that is reproduced by exercise, eating, and/or stress and is subsequently relieved with rest, and without recent change in frequency or severity of activity that produce symptoms, is called chronic stable angina. Over time, the plaques may thicken and rupture, exposing a thrombogenic surface upon which platelets aggregate and thrombus forms. The patient may note a change in symptoms of cardiac ischemia with a change in severity or of duration of symptoms. This condition is referred to as unstable angina.
Patients with STEMI have a high likelihood of a coronary thrombus occluding the infarct artery. Angiographic evidence of coronary thrombus formation may be seen in more than 90% of patients with STEMI but in only 1% of patients with stable angina and about 35-75% of patients with unstable angina or NSTEMI. However, not every STEMI evolves into a Q-wave MI; likewise, a patient with NSTEMI may develop Q waves.
The excessive mortality rate of coronary heart disease is primarily due to rupture and thrombosis of the atherosclerotic plaque. Inflammation plays a critical role in plaque destabilization and is widespread in the coronary and remote vascular beds. Systemic inflammatory, thrombotic, and hemodynamic factors are relevant to the outcome. Evidence indicates that platelets contribute to promoting plaque inflammation as well as thrombosis. A new theory of unbalanced cytokine-mediated inflammation is emerging, providing an opportunity for intervention.
A less common cause of angina is dynamic obstruction, which may be caused by intense focal spasm of a segment of an epicardial artery (Prinzmetal angina). Coronary vasospasm is a frequent complication in patients with connective tissue disease. Other causes include arterial inflammation and secondary unstable angina. Arterial inflammation may be caused by or related to infection. Secondary unstable angina occurs when the precipitating cause is extrinsic to the coronary arterial bed, such as fever, tachycardia, thyrotoxicosis, hypotension, anemia, or hypoxemia. Most patients who experience secondary unstable angina have chronic stable angina as a baseline medical condition.
Spontaneous and cocaine-related coronary artery dissection remains an unusual cause of ACS and should be included in the differential diagnosis, especially when a younger female or cocaine user is being evaluated. An early clinical suspicion of this disease is necessary for a good outcome. Cardiology consultation should be obtained for consideration for urgent percutaneous coronary intervention.
Although rare, pediatric and adult ACS may result from the following (see Myocardial Infarction in Childhood):
- ACS may occur with Marfan syndrome; Kawasaki disease; Takayasu arteritis; or cystic medial necrosis with aortic root dilatation, aneurysm formation, and dissection into the coronary artery.
- Anomalous origin of the left coronary artery from the pulmonary artery may occur as unexplained sudden death in a neonate.
- Coronary artery ostial stenosis may occur after repair of a transposition of the great arteries in the neonatal period.
- An aberrant left main coronary artery with its origin at the right sinus of Valsalva may cause ACS, especially with exertion.
- Traumatic myocardial infarction can occur in patients at any age.
- Accelerated atherosclerosis is known to occur in cardiac transplant recipients on immunosuppressive therapy.
- ACS may occur with progeria.
Irrespective of the cause of unstable angina, the result of persistent ischemia is myocardial infarction (MI).
Frequency
United States
Although the exact incidence of ACS is difficult to ascertain, hospital discharge data indicate that 1,680,000 unique discharges for ACS occurred in 2001.
International
In Britain, annual incidence rate of angina is estimated at 1.1 cases per 1000 males and 0.5 cases per 1000 females aged 31-70 years. In Sweden, chest pain of ischemic origin is thought to affect 5% of all males aged 50-57 years. In industrialized countries, annual incidence rate of unstable angina is approximately 6 cases per 10,000 people.
Mortality/Morbidity
When the only therapy for angina was nitroglycerin and limitation of activity, patients with newly diagnosed angina had a 40% incidence of MI and a 17% mortality rate within 3 months. A recent study shows that the 30-day mortality rate from ACS has decreased as treatment has improved, a statistically significant 47% relative decrease in 30-day mortality rate among newly diagnosed ACS from 1987-2000. This decrease in mortality rate is attributed to aspirin, glycoprotein (GP) IIb/IIIa blockers, and coronary revascularization via medical intervention or procedures.
Clinical characteristics associated with a poor prognosis include advanced age, male sex, prior MI, diabetes, hypertension, and multiple-vessel or left-mainstem disease.
Sex
Incidence is higher in males among all patients younger than 70 years. This is due to the cardioprotective effect of estrogen in females. At 15 years postmenopause, the incidence of angina occurs with equal frequency in both sexes. Evidence exists that women more often have coronary events without typical symptoms, which might explain the frequent failure to initially diagnose ACS in women.
Age
ACS becomes progressively more common with increasing age. In persons aged 40-70 years, ACS is diagnosed more often in men than in women. In persons older than 70 years, men and women are affected equally.
Clinical
History
- Typically, angina is a symptom of myocardial ischemia that appears in circumstances of increased oxygen demand. It is usually described as a sensation of chest pressure or heaviness, which is reproduced by activities or conditions that increase myocardial oxygen demand.
- Not all patients experience chest pain. Some present with only neck, jaw, ear, arm, or epigastric discomfort.
- Other symptoms, such as shortness of breath or severe weakness, may represent anginal equivalents.
- A patient may present to the ED because of a change in pattern or severity of symptoms. A new case of angina is more difficult to diagnose because symptoms are often vague and similar to those caused by other conditions (eg, indigestion, anxiety).
- Patients may have no pain and may only complain of episodic shortness of breath, weakness, lightheadedness, diaphoresis, or nausea and vomiting.
- Patients may complain of the following:
- Palpitations
- Pain, which is usually described as pressure, squeezing, or a burning sensation across the precordium and may radiate to the neck, shoulder, jaw, back, upper abdomen, or either arm
- Exertional dyspnea that resolves with pain or rest
- Diaphoresis from sympathetic discharge
- Nausea from vagal stimulation
- Decreased exercise tolerance
- Patients with diabetes and elderly patients are more likely to have atypical presentations and offer only vague complaints, such as weakness, dyspnea, lightheadedness, and nausea.
- Stable angina
- Involves episodic pain lasting 5-15 minutes
- Provoked by exertion
- Relieved by rest or nitroglycerin
- Unstable angina: Patients have increased risk for adverse cardiac events, such as MI or death. Three clinically distinct forms exist, as follows:
- New-onset exertional angina
- Angina of increasing frequency or duration or refractory to nitroglycerin
- Angina at rest
- Variant angina (Prinzmetal angina)
- Occurs primarily at rest
- Triggered by smoking
- Thought to be due to coronary vasospasm
- Elderly persons and those with diabetes may have particularly subtle presentations and may complain of fatigue, syncope, or weakness. Elderly persons may also present with only altered mental status. Those with preexisting altered mental status or dementia may have no recollection of recent symptoms and may have no complaints whatsoever.
- As many as half of cases of ACS are clinically silent in that they do not cause the classic symptoms described above and consequently go unrecognized by the patient. Maintain a high index of suspicion for ACS especially when evaluating women, patients with diabetes, older patients, patients with dementia, and those with a history of heart failure.
Physical
- Physical examination results are frequently normal. If chest pain is ongoing, the patient will usually lie quietly in bed and may appear anxious, diaphoretic, and pale.
- Hypertension may precipitate angina or reflect elevated catecholamine levels due to either anxiety or exogenous sympathomimetic stimulation.
- Hypotension indicates ventricular dysfunction due to myocardial ischemia, infarction, or acute valvular dysfunction.
- Congestive heart failure (CHF)
- Jugular venous distention
- Third heart sound (S3) may be present.
- A new murmur may reflect papillary muscle dysfunction.
- Rales on pulmonary examination may suggest left ventricular (LV) dysfunction or mitral regurgitation.
- Presence of a fourth heart sound (S4) is a common finding in patients with poor ventricular compliance due to preexisting ischemic heart disease or hypertension.
Causes
- Atherosclerotic plaque is the predominant cause. Coronary artery vasospasm is less common.
- Alternative causes of angina include the following:
- Ventricular hypertrophy due to hypertension, valvular disease, or cardiomyopathy
- Embolic occlusion of the coronary arteries
- Hypoxia, as in carbon monoxide poisoning or acute pulmonary disorders
- Cocaine and amphetamines, which increase myocardial oxygen demand and may cause coronary vasospasm
- Underlying coronary artery disease, which may be unmasked by severe anemia
- Inflammation of epicardial arteries
- Coronary artery dissection
- Risk factors for ACS should be documented and include the following:
- Male gender
- Diabetes mellitus (DM)
- Smoking history
- Hypertension
- Increased age
- Hypercholesterolemia
- Hyperlipidemia
- Prior cerebrovascular accident (CVA) - These patients constitute 7.5% of patients with ACS and have high-risk features.
- Inherited metabolic disorders
- Methamphetamine use
- Occupational stress
- Connective tissue disease
- Source: Emedicine.medscape






0 comments
Post a Comment
[▼/▲] More Emoticons